After bariatric surgery, the question is no longer whether you need lifelong vitamin supplementation — it is which delivery format will give your restructured digestive system the best chance of actually absorbing what it needs. The three dominant formats on the market today are chewable tablets, liquid softgel capsules, and traditional hard capsules or tablets. Each comes with trade-offs in bioavailability, compliance, gastric tolerance, and cost.
This comparison is not academic. Nutrient deficiencies following procedures like Roux-en-Y gastric bypass, sleeve gastrectomy, and duodenal switch are well-documented and, in some cases, irreversible. Choosing the wrong supplement format can quietly undermine even the most disciplined post-operative nutrition plan.
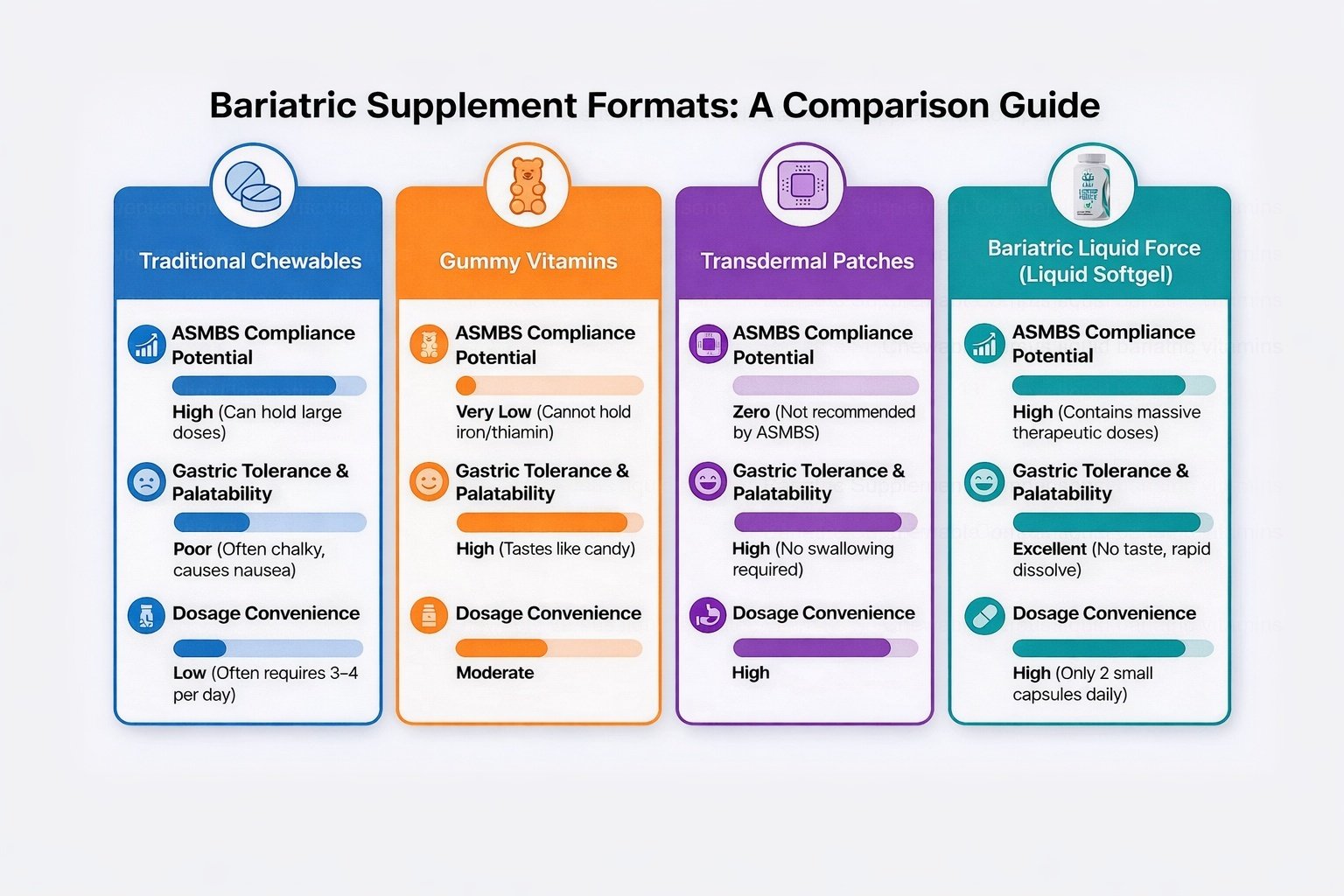
Liquid softgel bariatric vitamins generally offer the best combination of absorption, ASMBS compliance, gastric tolerance, and dosing convenience. Chewables remain a viable option but typically require more daily doses and may cause nausea in sensitive patients. Gummy vitamins and transdermal patches fall short of clinical standards and are not recommended as primary bariatric supplementation.
Why Absorption Format Matters After Bariatric Surgery
Bariatric procedures fundamentally alter gastrointestinal anatomy. Gastric bypass reroutes food past a significant portion of the small intestine — the primary site of micronutrient absorption. Sleeve gastrectomy removes roughly 80% of the stomach, drastically reducing both its volume and its acid production. These changes have a direct impact on how efficiently any given supplement format can deliver its nutrients into the bloodstream.
A standard multivitamin designed for someone with intact anatomy assumes a full stomach acid bath, normal transit time, and the entire length of the small intestine for absorption. None of those assumptions hold after most bariatric procedures. According to the American Society for Metabolic and Bariatric Surgery (ASMBS) nutritional guidelines, post-operative patients require specialized supplementation that accounts for these anatomical realities.
The supplement format — the physical vehicle that delivers nutrients to the gut — determines how quickly and completely those nutrients become available. A hard tablet must first disintegrate, then dissolve, then be absorbed. A liquid softgel eliminates the disintegration step entirely. A chewable sits somewhere in between: mechanically broken down by chewing, but still containing binders and fillers that must dissolve before the active ingredients are freed. When the available absorption window is shortened by surgery, every step that can be eliminated improves the odds of adequate nutrient uptake.
Format-by-Format Comparison
Liquid Softgels
Liquid softgel capsules contain nutrients already dissolved or suspended in an oil-based medium inside a gelatin shell. When the shell dissolves — which happens rapidly in the stomach — the contents are immediately available for absorption with no further disintegration required. This gives liquid softgels a meaningful pharmacokinetic advantage in patients with reduced gastric volume and lower acid production.
Research published in the Journal of Pharmacy and Pharmacology has demonstrated that liquid-filled capsules achieve higher peak plasma concentrations and faster time-to-peak compared with equivalent solid dosage forms. For bariatric patients whose absorption window is already compressed, this faster onset translates into more complete nutrient uptake.
From a compliance standpoint, high-quality liquid softgels can deliver a full therapeutic dose in just two capsules per day. They produce no chalky taste or texture, dissolve smoothly, and are associated with excellent gastric tolerance — a critical factor in the weeks and months following surgery when nausea sensitivity is at its highest. Liquid softgels that are specifically formulated for bariatric patients can meet the full scope of ASMBS micronutrient recommendations.
Traditional Chewables
Chewable vitamins were for many years the default recommendation after bariatric surgery, primarily because they do not require the same level of stomach acid as hard tablets for disintegration. The mechanical process of chewing begins the breakdown, giving them an advantage over swallowed tablets in a low-acid environment.
However, chewables carry well-known drawbacks. To fit meaningful doses of all required micronutrients into a chewable format, manufacturers typically require patients to take three to four tablets per day. This higher pill burden has a measurable negative impact on long-term adherence. A review of bariatric supplement compliance published in Obesity Surgery found that regimen complexity — particularly the number of daily doses — was among the strongest predictors of non-adherence over time.
Gastric tolerance is another concern. The binders and fillers required to hold a chewable tablet together create a chalky, sometimes gritty texture that many post-operative patients find nauseating. This is especially problematic in the first six months after surgery, when taste aversions and food sensitivities are most pronounced. Patients who experience nausea with their supplement are far more likely to skip doses or discontinue supplementation altogether.
That said, chewable bariatric vitamins from reputable manufacturers can and do meet ASMBS nutritional guidelines. For patients who tolerate them well and maintain a consistent multi-dose daily regimen, they remain a clinically acceptable option.
Gummy Vitamins
Gummy vitamins are the fastest-growing segment of the consumer supplement market, and their appeal is obvious: they taste good, feel more like a treat than a medical obligation, and have essentially zero texture issues. For the general population, they can be a reasonable way to fill modest nutritional gaps.
For bariatric patients, however, gummies present serious shortcomings. The gummy matrix — the gelatin, sugar, and flavoring base — takes up a large proportion of each unit's volume, leaving limited room for active ingredients. As a direct consequence, most gummy bariatric vitamins lack adequate doses of iron and thiamin (vitamin B1), two nutrients that bariatric patients are at particularly high risk of becoming deficient in. Iron deficiency can lead to anemia and chronic fatigue, while thiamin deficiency, though rarer, can progress to Wernicke encephalopathy — a potentially life-threatening neurological emergency.
ASMBS compliance for gummy vitamins is effectively zero when it comes to the full spectrum of post-bariatric nutritional needs. They may serve as a palatable supplement for one or two specific nutrients, but they should not be relied upon as a patient's primary multivitamin after weight loss surgery.
Transdermal Patches
Vitamin patches applied to the skin represent the newest entrant in the bariatric supplement market. Their appeal is entirely about convenience — no swallowing, no taste, no gastrointestinal involvement at all. In theory, bypassing the gut entirely would sidestep all the absorption challenges created by bariatric surgery.
In practice, the evidence does not support this theory. Transdermal delivery works well for certain small-molecule drugs (nicotine, estrogen, nitroglycerin) but faces significant challenges with the large, diverse array of vitamins and minerals that bariatric patients need. Many micronutrients are too large or too hydrophilic to cross the skin barrier efficiently. To date, no transdermal vitamin patch has received ASMBS compliance recognition, and the clinical research supporting their efficacy in bariatric populations remains extremely thin.
While patches score high on convenience and gastric tolerance (since they bypass the stomach entirely), their zero ASMBS compliance means they cannot currently be recommended as a stand-alone supplementation strategy after bariatric surgery.
The Bioavailability Question: What Does the Research Say?
Bioavailability — the proportion of an ingested nutrient that reaches systemic circulation — is the central metric in this debate. A vitamin that scores perfectly on paper but only delivers 30% of its stated dose into the bloodstream is, in functional terms, a 30% vitamin.
Several factors influence bioavailability after bariatric surgery. The first is disintegration time: how quickly the physical dosage form breaks apart in the stomach. Hard tablets can take 30 minutes or more to disintegrate, a timeframe that may exceed the transit time through a gastric pouch. Chewables disintegrate faster because chewing provides the initial mechanical breakdown, but the binder matrix still needs to dissolve. Liquid softgels bypass disintegration almost entirely.
The second factor is the biochemical form of each nutrient. Iron bisglycinate, for example, is absorbed through a different intestinal pathway than ferrous sulfate, making it less dependent on stomach acid. Methylcobalamin (a form of B12) is more readily absorbed than cyanocobalamin. These formulation-level details matter as much as, or more than, the physical format — which is why it is important to look beyond the delivery vehicle and examine the actual ingredient list of any bariatric supplement.
The third factor is dosing frequency and compliance. A theoretically superior formulation that a patient takes inconsistently will deliver worse outcomes than a moderately bioavailable formulation taken reliably every day. This is where the convenience advantage of two-per-day liquid softgels over three-to-four-per-day chewables becomes clinically meaningful: over months and years, the simpler regimen tends to win.
ASMBS Guidelines and What They Mean for Format Choice
The ASMBS publishes detailed nutritional guidelines specifying the minimum daily intake of key micronutrients for each type of bariatric procedure. These guidelines are the clinical gold standard, and any bariatric vitamin worth considering should be formulated to meet or exceed them.
It is important to understand that ASMBS guidelines specify nutrient amounts, not delivery formats. The Society does not officially endorse liquid softgels over chewables or vice versa. What it does endorse is the practice of choosing supplements specifically designed for bariatric patients, avoiding standard over-the-counter multivitamins, and monitoring bloodwork regularly to confirm that the chosen regimen is actually maintaining adequate levels.
That said, format influences whether a product can meet ASMBS standards. As noted above, gummy vitamins typically cannot accommodate the required iron and thiamin doses. Patches lack the clinical validation to confirm that their transdermal delivery achieves blood levels equivalent to oral supplementation. Chewables and liquid softgels, when properly formulated, can both meet ASMBS thresholds — but the compliance advantage of the lower-dose-count softgel format may help patients maintain those levels more consistently over time. For a deeper look at the full landscape of bariatric vitamins after weight loss surgery, including what to look for on a label, our comprehensive guide covers the essentials.
Bari Liquid Force is a two-per-day liquid softgel bariatric multivitamin formulated to meet ASMBS nutritional guidelines, with high-absorption nutrient forms and no chalky taste or texture.
Learn More About Bari Liquid Force →60-day money-back guarantee · Free shipping with Prime
Making the Right Choice for Your Situation
There is no universal "best" format for every bariatric patient, because individual factors — procedure type, time since surgery, personal tolerance, budget, and adherence patterns — all play a role. What the evidence does support is a clear hierarchy of reliability.
Liquid softgels occupy the top tier for most patients because they combine rapid dissolution, high bioavailability, strong gastric tolerance, low pill burden, and demonstrated ability to meet ASMBS guidelines. They are particularly well-suited for patients in the early post-operative period when nausea sensitivity is highest and establishing a consistent supplement habit is most critical.
Chewable tablets remain a solid second option, especially for patients who prefer the ritual of chewing and have no issues with taste or texture. The key trade-off is the higher number of daily doses required. Patients who choose chewables should pay close attention to adherence: if they find themselves routinely skipping the third or fourth dose of the day, the theoretical nutrient content on the label is not reaching their bloodstream.
Gummy vitamins and transdermal patches, despite their appeal, are not appropriate as primary bariatric supplementation at this time. Gummies can serve as a pleasant-tasting complement for specific nutrients (like vitamin D) but should not replace a comprehensive bariatric multivitamin. Patches may hold future promise as transdermal technology advances, but the current evidence base is insufficient to recommend them with confidence.
A Note on Monitoring
Regardless of which format you choose, regular blood work is non-negotiable. The ASMBS recommends comprehensive micronutrient panels at baseline, three months, six months, twelve months, and annually thereafter. These labs are the only way to confirm that your chosen supplement is actually maintaining adequate levels. A format that works well for one patient may underperform for another due to individual variations in absorption, metabolism, and dietary intake.
If bloodwork reveals a deficiency despite consistent supplementation, the first question to explore with your bariatric team is whether a format change or a dose adjustment might resolve the issue before adding standalone supplements. Simplifying the regimen wherever possible supports the long-term adherence that ultimately determines outcomes.